The Painful Truth: All About Endometriosis

Let’s talk “endo” guys. Endometriosis is a gynecologic condition that occurs in 6–10% of women of reproductive age, with a prevalence of 38% (range, 20–50%) in infertile women. According to studies, there appears to be no particular racial predisposition to endometriosis. I believe the reason why we might see a growing number of endometriosis cases in black women is likely secondary to an increase in awareness, and thus, more women seeking out diagnosis now more than ever.
The main causative factor is complex but is still thought to be principally associated with an overproduction of local estrogen by increased aromatase activity with subsequent attachment and implantation of endometrial glands and stroma on the peritoneum from retrograde menstruation. So WTF does that mean? Lol 🤣 This is fancy terminology that means: You have so much estrogen that the shed lining from the uterus flows from inside the uterus backwards through the Fallopian tubes, and into the abdominal cavity (below).

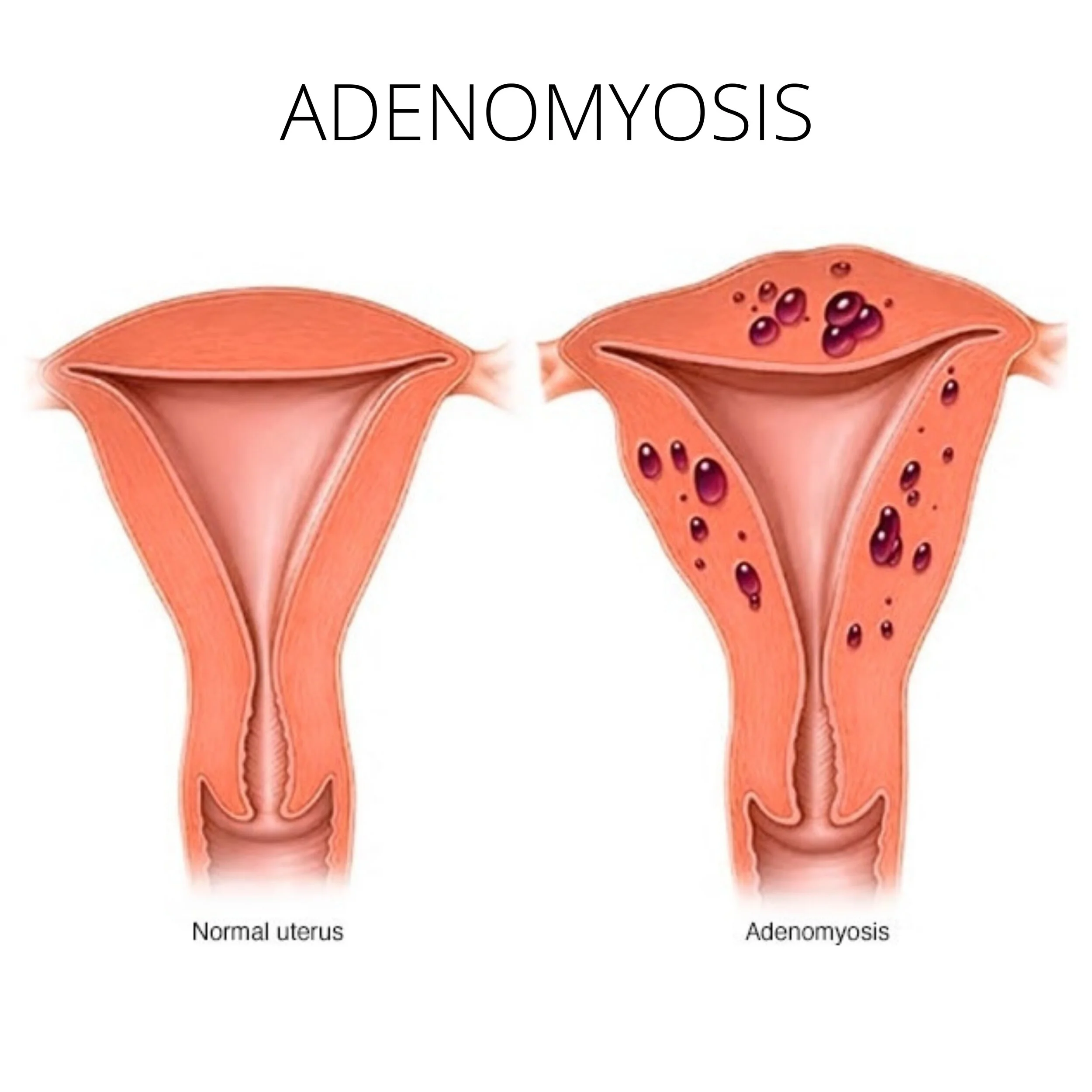
The lining can also flow backwards into the uterine muscle. When this happens, it is called adenoomyosis. So that’s right! Adenomyosis, is a form of endometriosis (below).
Please also know that this condition does have a genetic component! Patients with an affected first-degree relative (mom, sister, or daughter) have nearly a 7–10 fold increased risk of developing endometriosis!
So what causes all this doggone pain during your period? The pain is due to an overproduction of prostaglandins and cytokines by an increase in cyclooxygenase-2 (COX-2) activity. These chemicals can lead to scar tissue formation in the pelvis, causing the following symptoms:
⚠️ Dysmenorrhea (pelvic pain during menses)
⚠️ Back pain during menses
⚠️ Chronic pelvic pain (pelvic pain > 6 months in duration)
⚠️ Dyspareunia (pain during sex)
⚠️ Uterosacral ligament nodularity (ask your doctor to perform a rectal exam during your evaluation to appreciate this! A lot of us OBGYN’s forget this step!)
⚠️ Large ovarian cyst known as an Endometriomas
⚠️ Constipation and painful bowel movements if the implants are on your rectum
⚠️ Infertility
Infertility is caused as the scar tissue cause kinking of the Fallopian tubes, so the egg cannot travel to and implant in the uterus; 30 to 50% of women with endometriosis are infertile, so even though the risk is significant, having endometriosis does not mean that you automatically can’t have children!


In order to help your doc diagnose this disease effectively, start keeping a food and pain diary as noted above This helps us to make sure you don’t have any other issues causing your symptoms, like irritable bowel syndrome, or bladder conditions.
Unless in the case of adenomyosis, these implants cannot be seen on ultrasound. The definitive diagnosis of endometriosis only can be made by biopsy and testing of lesions removed at laparoscopic surgery (below).

HOWEVER, surgery is NOT necessary in order to start treatment, especially if your symptoms align with several of those listed above and you tend to have a classic presentation of endometriosis. Just know that if you are being treated without surgery, this doesn’t CONFIRM that you have endometriosis, it would only be a suspicion.
As far as treatment goes, much like anything else, we gotta decide if you want kids or not.
If you don’t want children and you are > 65 years, removing the uterus AND the ovaries are your best bet. The ovaries are responsible for producing this extra estrogen wreaking havoc, so they gotta go! If you leave your ovaries, there is a 62% likelihood of recurrent symptoms, while only 10% if they are outta there!
If you don’t want children and you are < 65 years, you can still have a hysterectomy, but if you are extremely young, you may want to consider keeping your ovaries a while, as they decrease your risk for all-cause mortality. But, as you can imagine, they will still continue to produce estrogen, so there is a chance that you may have a recurrence of symptoms.
If you want kids, your options include:
💊 Oral progestins, Progesterone IUD, or birth control pills to balance out the estrogen
💊 Oral danazol to decrease androgen-stimulated pain
💊 Nonsteroidal anti-inflammatory drugs [NSAIDS] like ibuprofen and naproxen to decrease the prostaglandins and cytokines that lead to scar tissue formation
💊 Depo Lupron to shut down your ovaries from making estrogen for a few months. You can only use this for up to a year. This medication puts you into menopause and can cause hot flushes, vaginal dryness, mood swings, and osteoporosis. Make sure your doc puts you on an oral progestin (if you are a candidate) while taking Depo Lupron to combat the osteoporosis risk if you plan to be on this med long-term.
Of course, a recurrence of symptoms is common after the medication is discontinued. Some of these recurrence rates can be as high as 50-70%.

How an HSG and Chromopertubation works
Surgical management includes removing as many lesions and scar tissue as possible. Ask about chromopertubation (above) if you have concerns for infertility to determine if your tubes are open.
Surgical management of endometriosis-related infertility does improve pregnancy rates, but the magnitude of improvement is unclear. If you are noted to have deeply infiltrating lesions during surgery, in vitro fertilization for pregnancy is going to be your best bet. If you have an endometrioma, studies have shown that the pregnancy rate was 60.9 % after excision versus 23.4% with the drainage and ablation technique, so ask your doc to try as hard as it is safely possible to excise the cyst, and not just drain it if you struggle with fertility.
Younger patients having a higher probability of re-operation for symptoms in their future.
Regarding pain management, Imma keep it real with y’all: WE SUCK. With this “opioid crisis” and strict regulations against prescribers, getting pain relief with endometriosis is difficult. So below are my recs for this:
1️⃣ Keep a diary as noted above. Whenever you figure out a timing pattern for your pain, start taking your ibuprofen SCHEDULED (if no contraindications) 3 days prior to suspected pain inception date.
2️⃣ Ask your doctor about other available NSAIDs. To be honest, a lot of us don’t work outside of ibuprofen and naproxen. BUT THERE ARE SO MANY OTHERS, like diclofenac, Celebrex, and mefenemic acid. Inquire about these to see if you are a candidate.
3️⃣ I tell my patients to rotate between your NSAID above and Tylenol every 3-4 hours if medically able.
4️⃣ Experiment with cold and heat therapy
5️⃣ Experiment with Kegels (below)

6️⃣ TAKING DIARY OUT OF MY DIET DID WONDERS for my cramps. Remember, there is a lot of hormonal use with animals now-a-days, so you could potentially be worsening your cramps if you’re still ingesting cow’s milk.
7️⃣ Ask for a work note if your pain is too debilitating for you to work. I know I’m always happy to provide one, and I’m sure other OBGYNs will be too.
8️⃣ Experiment with pelvic floor physiotherapy
9️⃣ If, and only if, you fail to see improvement as that above and you don’t have a history of or risk factors for narcotic abuse, ask your physician about a small prescription for a narcotic. If you don’t have a history of narcotic abuse, ask them to check whatever prescription monitoring program they use to ensure you haven’t had an extensive history for narcotic abuse or prescriptions; for Texas, it’s Texas PMP Aware. If you have an extensive history of narcotic use and prescriptions, I can’t help you here. If not, a 1 time prescription shouldn’t hurt, but this is up to your doctor’s comfortability level and he/she/they shouldn’t be demonized or coerced into filling anything. B/c narcotics do cause bowel and other issues, you should limit your narcotic use to only a couple days (you severest days) out of the month, and you shouldn’t need to use more than 10-12 pills every few months.
Endo is a DOOZY! I understand your pain and struggle. I truly hope this helps someone out there. Next week, we’ll discuss PCOS! 🤗